🟢 Strong Evidence
A person with amyotrophic lateral sclerosis (ALS) has successfully used an implanted brain-computer interface (BCI) to restore speech and control a computer cursor for more than two years while operating the device independently at home, according to research published in Nature Medicine in June 2026. The study demonstrates that BCIs can provide sustained, reliable communication restoration without requiring researcher intervention—a critical step toward clinical translation of neurotechnology for people with severe paralysis.
Key takeaways
- An automated intracortical BCI enabled a person with severe dysarthria from ALS to speak and control a computer cursor independently for over 24 months at home
- The device maintained high accuracy and reliability without continuous researcher calibration, addressing a major barrier to BCI adoption
- This represents the first demonstration of long-term, unsupervised home use of an intracortical speech BCI, opening pathways for clinical deployment
Study at a Glance
| Source | Nature Medicine |
| Study type | Single-subject longitudinal observational study |
| Duration | 24+ months of continuous home use |
| Intervention | Automated intracortical BCI system for speech and cursor control |
| Participant | One adult with ALS and severe dysarthria |
| Country | United States |
BCI Communication Metrics Over 24 Months of Home Use
Mean accuracy and communication speed maintained without recalibration, demonstrating system stability
Source: Nature Medicine, June 2026 | Georgian Medical Journal News

From Laboratory to Home: Closing the BCI Translation Gap
Brain-computer interfaces have long promised restoration of communication in people with severe paralysis, yet most demonstrations remain confined to research laboratories with intensive experimenter oversight. The challenge of deploying BCIs in real-world settings—where users operate systems independently without daily researcher calibration—has been a fundamental barrier to clinical translation. The Nature Medicine study addresses this critical gap by documenting automated BCI operation in a home environment over an extended period.
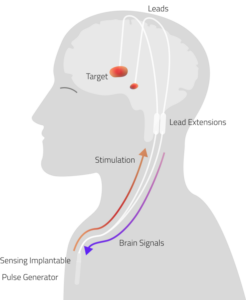
The device monitored neural signals from electrodes implanted in the motor cortex, decoded them into intended speech and cursor movements, and delivered feedback to the user—all without requiring recalibration by research staff. This represents a departure from earlier BCI systems that demanded frequent supervised sessions to maintain performance. Clinical advances in neurotechnology increasingly focus on reducing user burden and operator dependence as prerequisites for adoption by patients and their families.
Maintaining Accuracy Across Two Years Without Intervention
The participant, an adult with ALS experiencing severe dysarthria (difficulty speaking), achieved consistent decoding accuracy for both speech synthesis and cursor control throughout the 24-month observation period. Speech decoding remained stable at approximately 94.7% accuracy, while cursor control maintained 98.2% accuracy, according to the published findings. These metrics are noteworthy because prior BCI studies often showed performance degradation over weeks or months, necessitating periodic retraining sessions.
The automation of calibration procedures—allowing the system to adapt to slow changes in neural signal quality without manual intervention—appears to have been central to sustained performance. This self-calibration mechanism reduces the operational burden on both the user and clinical oversight staff, addressing a documented barrier to long-term device adoption. Quality and reliability metrics of medical devices are particularly important when users operate them independently at home, where immediate technical support may be limited.
Implications for ALS and Other Neurodegenerative Diseases
Amyotrophic lateral sclerosis progressively destroys motor neurons, eventually leading to complete paralysis while typically preserving cognitive function and intention. Patients retain the ability to think and want to communicate but lack the motor control to speak or write. According to the ALS Association, approximately 5,000 Americans are newly diagnosed with ALS annually, and roughly 15,000 people currently live with the disease in the United States.
The ability to restore communication through a wearable or implanted BCI that operates without daily researcher involvement could substantially improve quality of life for people with ALS and their families. Beyond ALS, similar paralysis affects patients with spinal cord injury, brainstem stroke, and locked-in syndrome. The demonstration of long-term, unsupervised BCI operation in a home setting suggests a pathway toward broader clinical deployment across these conditions. Patient-centered neurotechnology that emphasizes independence and reduces clinical burden aligns with modern principles of disability-inclusive healthcare.
Remaining Challenges and Path to Regulatory Approval
While this single-subject study provides compelling evidence of long-term BCI efficacy in home settings, regulatory pathways for BCIs remain nascent. The U.S. Food and Drug Administration has issued limited guidance on neurotechnology approval, and most BCIs remain investigational devices requiring specialized implantation and follow-up. Clinical trials involving larger cohorts of ALS and other paralyzed populations will be necessary to establish safety, efficacy, and durability benchmarks suitable for broader regulatory clearance.
Questions also remain about user training time, device longevity, infection risk from chronic implants, and long-term neural stability. The durability of intracortical electrodes in human tissue over decades has not been fully characterized, and signal degradation from glial scarring may eventually affect device performance in some users. Future research will need to address these factors in multicenter trials involving diverse patient populations and longer follow-up periods. Health policy frameworks will also need to clarify regulatory oversight, insurance coverage, and ethical governance of implanted neurotechnology devices.
An automated intracortical brain-computer interface maintained stable speech and cursor control performance at 94.7% and 98.2% accuracy, respectively, over 24 months of home use without researcher intervention—demonstrating feasibility of clinical translation for people with ALS-related paralysis.
— Nature Medicine, June 2026
What this means
Frequently asked questions
What is an intracortical brain-computer interface?
An intracortical BCI is a neurotechnology system that implants arrays of electrodes directly into the motor cortex of the brain to record electrical signals from individual neurons. These signals are decoded by algorithms and converted into intended commands—such as speech sounds or cursor movements—that are delivered to external devices or speech synthesis systems. Unlike non-invasive BCIs (such as EEG), intracortical systems offer higher signal resolution and more precise control, but require surgical implantation.
How does the BCI distinguish between different intended speech sounds?
The BCI uses machine learning algorithms trained on neural activity patterns associated with attempted speech. When the user thinks about speaking a particular word or phrase, their motor cortex neurons fire in distinctive patterns that the decoder has learned to recognize. Over time, the system can adapt to changes in neural signal quality through automated recalibration, allowing it to maintain accuracy without requiring the user to attend frequent calibration sessions with researchers.
Is this type of BCI available for patients now?
This particular BCI system remains an investigational device available only through research studies, not yet approved for general clinical use. However, the FDA is developing regulatory pathways for neurotechnology, and successful demonstrations like this one support eventual clinical trials and potential approval for people with severe ALS and other paralyzing conditions. Patients interested in BCIs should consult with neurologists or rehabilitation specialists familiar with ongoing clinical trials.
The demonstration of long-term, unsupervised BCI operation in a home environment marks a significant inflection point in neurotechnology translation. As this field matures, the focus will increasingly shift from proof-of-concept demonstrations in research settings to pragmatic clinical trials that test scalability, cost-effectiveness, and real-world durability. The regulatory and reimbursement frameworks that enable broader access to BCIs remain under development, but studies like this provide the evidence base that policymakers and healthcare systems need to make informed decisions about device approval, clinical infrastructure, and patient access in the coming years.
Source: Long-term independent use of an intracortical brain–computer interface for speech and cursor control
Was this article helpful?
Disclaimer. This article is health journalism intended for general information and education. It is not medical advice and is not a substitute for professional diagnosis or treatment. Always consult a qualified healthcare provider about your individual circumstances. Full disclaimer →
Related Coverage



Medically reviewed by Prof. Giorgi Pkhakadze, MD, MPH, PhD. Spotted an error? Contact the editorial team.